

By Ray Goodspeed
The last week has seen an orgy of spiteful glee from the conservative right and their allies in the right-wing media as they claim to be vindicated by the final publication of the “Independent review into gender identity services for children and young people” in England and Wales by Dr Hilary Cass. Trans people, especially children and adolescents, now face more fear, anxiety and distress about the future.
Lurid claims have been made, that a generation of young people have been experimented on – sacrificed on the altar of a crazed “gender ideology” – and subjected to damaging, life-changing medical procedures on the basis of no evidence. Calls have been made for those who have supported trans rights to apologise, and it is clear that a fully-fledged witch-hunt is gathering pace. Already, the Scottish government has been pressured into implementing the Cass Review recommendations.
Hilary Cass herself is very careful to use warm words and sympathetic phrases about aiming for a “high quality of care”, a reduction of the long and multiple waiting lists, a “holistic” approach to dealing with the range of a child’s complex needs, and so on. In spite of such soft tones, however, the review is permeated by underlying assumptions which have been promoted by anti-trans campaigners. Moreover, its methodology was biased against research findings that do not fit into its unspoken aims – which are to severely restrict and reduce the available medical treatment for trans young people.
The Cass Review was set up in 2020 in response to growing controversy surrounding the Gender Identity Development Service (GIDS) based at the Tavistock and Portman NHS Trust in north London. GIDS was set up back in 1989, and until last month, it was the only service for trans or gender non-conforming children, taking referrals from all over in England and Wales (there is a separate centre in Scotland).
It offered counselling and psychotherapeutic services in addition to being able to authorise, in a minority of cases, medical interventions, primarily puberty blockers and, for those over 16, hormone replacement therapy, to ease transition and alleviate dysphoria – the discomfort and/or mismatch between your physical body and your gender identity. No surgery is carried out to under-18s – that is illegal in the UK.
Tavistock/GIDS in the centre of a storm
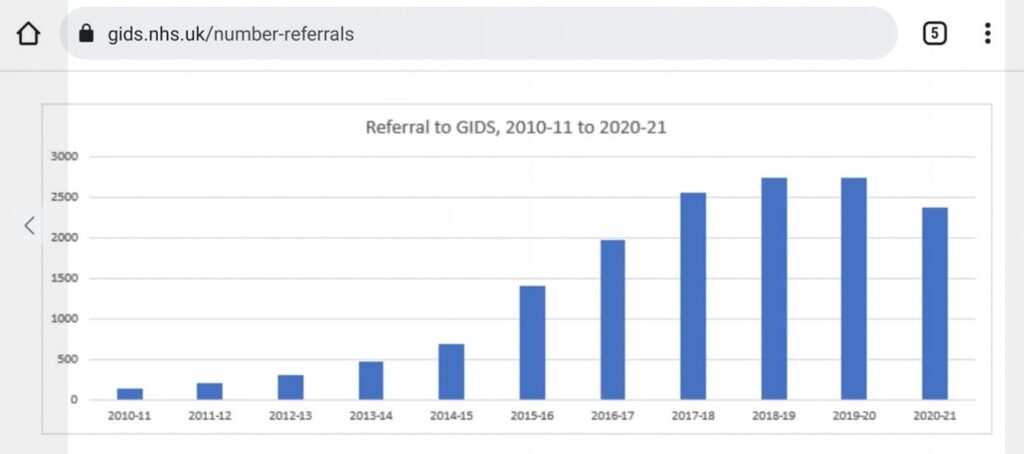
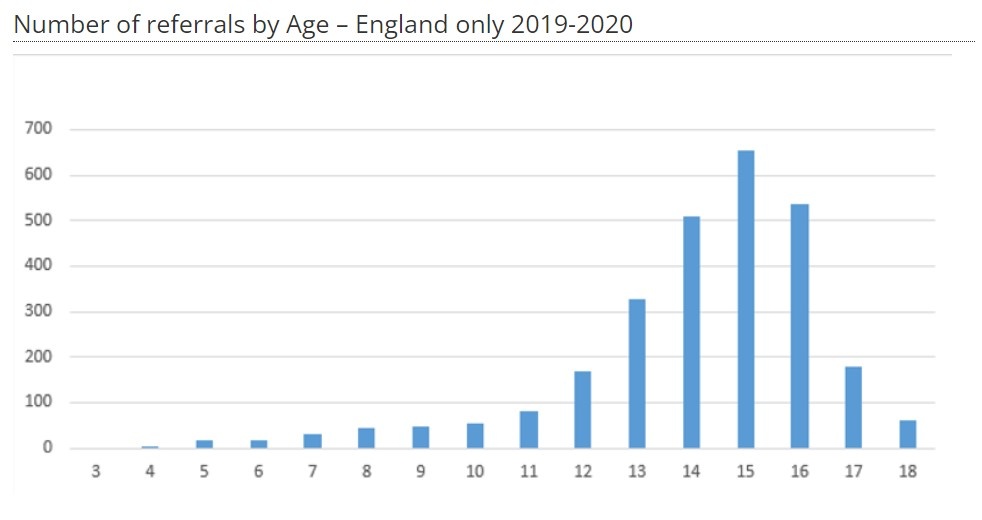
From about 2016 onwards GIDS became the centre of a storm about how to treat trans kids, caused by different interlocking factors. Firstly, the numbers of young people being referred to it rose very dramatically, particularly between 2016 and 2019-20, leading to the GIDS service being overwhelmed and to a huge increase in waiting times to access the service. At the time the Cass review was commissioned, in 2020, the waiting time was two years for a first appointment! The vast majority of referrals was for clients aged 13 and over and especially 14-16 year-olds.
The increase in referrals in the late 2010s coincided with so-called “peak-trans” – when trans people and issues became represented in the popular media more than ever before. Since 2019-20 the number of referrals has hit a plateau and more recently has actually started to dip.
Within these figures there was a significant increase in the proportion of “girls” (ie trans boys) being referred, compared to “boys” (ie trans girls). Part of the anti-trans backlash that gained strength at the same time was the claim from the conservative right, and some of their allies who identify as feminists, that these “girls” were not actually trans, but were victims of “social contagion” from peers and internet influencers.
This idea, so-called “Rapid Onset Gender Dysphoria”, was based on “research” that has been thoroughly discredited, and disowned even by the university that first published it. It was not based on any study of trans people, but solely on a survey of a couple of hundred of their parents who volunteered for the study and who were already members of anti-trans websites and chat groups! Subsequently, more reputable studies have shown there to be no evidence for this theory but it has nonetheless still been widely quoted by anti-trans campaigners. [More information on this theory and its refutation can be found here and here.]
With the increasing visibility of trans people, greater social acceptance and legal rights, and access to a community, both on the internet and in “real life”, the number of young people realising they are trans has increased. This has boosted the confidence and reduced the isolation of members of a tiny minority community. The exact same thing happened in the 70s and early 80s with lesbians and gay men, after male homosexuality was partially legalised in England and Wales in 1967. This was also subsequently followed by an intense period of hate-fuelled backlash.
Transphobia, sexism and misogyny
The relative increase in numbers of “girls” (trans boys) could reflect the much greater stigma that is associated with being trans women, who often bear the brunt of the worst transphobia, sexism and misogyny. It is much more socially acceptable for women to dress in a masculine or androgynous way, than for a man to wear “women’s clothes”. In the last century, nearly all the most famous cases of “transsexuals” having “sex-change” operations that were covered in the media involved trans women. Trans men were much less visible, and for many people, even the possibility that trans men existed was largely unknown. So with greater visibility, a more recent increase in the numbers of trans boys and men is to be expected.
A further talking point of the backlash was the statistically significant correlation between trans identity and autism or other forms of neuro-diversity, and the fact that many young people referred to GIDS also manifest symptoms of anxiety, depression, or even eating-disorders or previous trauma. The correlation with neuro-diversity would be an important field of research but no causal link has yet been demonstrated in either direction. And why should that future research prevent neuro-diverse young people from recognising their gender identity or acting upon it?
Of course, no reasonable person would say that a counselling service should not look at a child’s or an adolescent’s needs holistically, to examine how their various mental health problems interact. Gender clinicians would seek to do that. Being trans is not easy. Many or most trans children and adolescents will suffer from depression or anxiety linked to their trans identity and may be bullied or treated badly, even by family members. Suicide rates are higher than the non-trans average.
2019-20
But to say, as many anti-trans campaigners do, that exhibiting these symptoms necessarily suggests that they are not trans at all but “just depressed” and that the treatment for depression should replace treatment for their gender dysphoria is another matter entirely.
Ironically, the same anti-trans campaigners will argue that trans adolescents are really just gay or lesbian, but “decide” to be trans as a way of courting popularity, because life is easier being trans than homosexual! This is delusional nonsense, completely out of touch with the reality of the lives of trans youngsters. Moreover it fails to recognise the awkward fact that many trans people are not homosexual before they transition in any case!
Affirming trans identity
All of these issues were reflected in a dispute among clinicians within GIDS itself. While being the only non-private source of gender-related health care, it also operated as a gate-keeper, an obstacle which many trans people needed to overcome in order to get the treatment they wanted. The majority of its staff were committed to the general international medical and psychological consensus of “affirming” the trans identity of the patient while talking through all the interrelated issues, and the use in some cases of medical treatment, such as puberty blockers or, for over-16s, hormone treatments.
However, a minority of staff were sceptical, and some openly hostile, to this approach, and were much more reluctant to accept that a young person exhibiting mental health difficulties was trans, or to prescribe medication. Many of the latter became so-called “whistleblowers” and resigned from GIDS. This kind of pressure directly led to the Cass Review.
It is true that the GIDS clinicians at the Tavistock were working under enormous stress in a unique but under-funded service, overwhelmed by the huge and growing waiting list and vilified on a daily basis in the media. It is also true that many of their young clients, by the time they were first seen, had been sitting abandoned on a waiting list for years in increasing distress and frustration, while any accompanying mental health issues were not being addressed. They were often desperate for treatment. Cass herself recognises that this is most dangerous time for these young people, in terms of self-harm or suicide. GIDS staff had the difficult task of balancing all these pressures.
Cass could have used the review to help to support the staff with resources, to help provide the “high standard of care” that she says she desires, to reduce the waiting lists and allow staff to deal with clients in a more timely and thorough way. Some of the recommendations, in the abstract, are useful steps forward, if they are ever implemented, but the review as a whole shows its bias and sadly panders to all the anti-trans talking points. The GIDS service, rather than being enhanced, has been dismembered.
GIDS closed down
In 2022, Cass’s Interim Review proposed that the GIDS at Tavistock be simply closed down from 2023. The proposal was to replace it with eight regional centres. That would, on the face of it, have been a great improvement. But the first two new centres, at Great Ormond Street in London and Alder Hey in Liverpool did not open on time. So GIDS had to limp on for another year, taking no new referrals, extending the waiting list for a first appointment to an unbelievable five years – for a service for adolescents! It is expected that the next centre to open will be in Bristol but there is no target date. In the context of Tory underfunding of the NHS, the promised new service may never actually fully materialise.
GIDS was replaced by two regional centres in April this year, but instead of the 80 clinicians who worked at the Tavistock, with decades of expertise working with trans or gender non-conforming young people, the new service has only 18 clinicians, who do not have specific experience or expertise in the field.
on a Newcastle Demo against a transphobic event
(photo Davy Ellis)
They have had a serious problem in recruiting staff. Many Tavistock staff have gone elsewhere to avoid the stress of constant demonisation, but in any case, Cass recommended that the new service should not employ full-time “gender specialists” but generic paediatricians or psychologists. This has been touted as providing a “holistic” service catering for all the needs of the children, in multi-disciplinary teams. So why do gender specialists not have a place in those teams?
It is clear, once you get past the saccharine phrases, that the new service, to the extent that it will exist at all, will prioritise dealing with emotional and mental health problems, not as part of affirming the child’s trans identity but in the expectation (and secretly in the hope) that the number of trans young people will be much smaller in future.
Cass is very careful, of course, to say that the intention of the treatment, counselling etc will not be to “change” the child’s trans identity. She wants to avoid accusations of undertaking conversion therapy. She says the children should be “listened to”, and their “feelings” believed. All well and good. But the underlying beliefs informing the Cass Review are that the discredited social contagion theory is valid and that the number of trans people should ideally fall.
Puberty blockers
The issue of puberty blockers was a major feature of the vitriolic attack on GIDS. The accusation was that blockers were untested, experimental drugs that could inflict irreversible harm on children. Cass commissioned a review of the available research regarding the benefits of prescribing puberty blockers and it is in the methodology of this review that her bias is most evident.
There are countless studies, the world over, that attest to the psychological benefits of affirmative therapy and the use, in some cases, of puberty blockers. They have been used since the 1980s, initially to treat early-onset puberty in young children, but also to pause puberty for some trans adolescents to prevent the development of secondary sex characteristics that cause particular distress. If the young person stops taking them, puberty then recommences in the normal way.
As with many medications, there are issues that require careful supervision. Calcium supplements may be needed as hormones play a role in the development of bone density, though if blockers are stopped or if sex hormones (testosterone or oestrogen) are later prescribed, this problem is resolved. Future fertility also needs to be monitored and there is a possibility of problems with any future gender-affirming genital surgery that trans women may later require. All these factors need to be weighed up and discussed between the doctor, the young person and their parents or carers.
However, the overwhelming international scientific consensus is that, on balance, blockers can be a useful tool to treat extreme cases of gender dysphoria in adolescents. GIDS had an international reputation for caution. Cass audited 3,499 cases dealt with by GIDS. She found that only 27 percent of clients are referred for hormonal treatment, after six or seven appointments, and of these, just 54 percent received a prescription. Only around 100 children are currently taking blockers in England and Wales, and only around 1,000 over the last ten years.

To arrive at her conclusions, the Cass Review firstly ignored any study not in the English language. Then, out of 103 studies she simply discounted 101 that showed psychological benefits of blockers because they were not “high enough quality”, leaving two that show that the evidence of benefits is inconclusive and not proven. She accepted that studies in this field were “difficult”. But the issues involved in such studies are much more serious than that.
Unethical
Many of the studies she dismissed were rejected because they were not “double-blind” studies with a control group. But with puberty blockers, it would be entirely unethical, not to say pointless, to carry out such experimental tests. It would involve giving some children a placebo, a substance that does nothing, while other children get the blockers. But it would soon be obvious which ones had the placebo, as physical changes do or do not start to happen! Or maybe she would like some children who desperately want blockers to be denied them solely for the sake of the experiment!
The ethical problems of carrying out such tests on children are the precise reason why so many medicines are prescribed to children “off-label” ie for purposes other than those for which they are originally developed. This is not at all unusual. Cass is trying to hold puberty blockers to a higher standard of proof than other medicines for children in order to pursue her own biased agenda. Many other jurisdictions, most recently that of Germany, operate an approach based on the medical consensus of those working in the field, making use of their years of clinical experience.
Even Cass herself accepts that for some (few) cases puberty blockers may be the correct path to take, much to the frustration of some of her far-right cheerleaders. Likewise with hormone treatments for 16-18 year-olds, she urges extreme caution, but stops short of an outright ban. A court case (Bell vs Tavistock) that sought a legal ban was seen off by the Tavistock at the Court of Appeal, yet NHS England still continued to severely restrict the prescribing of blockers. Cass recommends that any child receiving puberty blockers must do so only as part of a research project, but making medical treatment conditional to agreeing to take part in research is, in itself, ethically dubious.
Cass suggests that the fact that 98 percent of those who are prescribed blockers go on to medically transition with sex hormone treatment is evidence of some automatic process towards full transition. But isn’t it more likely that if blockers are prescribed in the most extreme cases of dysphoria, those with the greatest distress, then they are exactly the young people who are likely to go on and medically transition?
Remarkably low regret rate
The true test of trans-affirming medical care is the vast number of trans people who recognise the benefits to their life of living in their true gender. Proof of this is the tiny percentage of those who detransition. Less than two percent of trans people stop transitioning or detransition, and of those, around half do so because of lack of family, community or financial support. Some re-transition later. The regret rate for trans surgery is less than one percent.

Each detransitioning case, of course, is a personal tragedy and they all deserve counselling, support and medical help if need be. But to restrict and reduce access to gender-affirming treatment on the basis of such a remarkably low regret-rate, much lower than for many other surgical procedures, is unfair and oppressive to the vast majority. Anti-trans campaigners have given a platform to the few detransitioners out of all proportion to their numbers. Yet, of the 3,499 cases looked at by Cass, the number who went on to detransition was a mere ten!
Cass recommends that younger children who want to socially transition, ie change their hair, clothes, name and so on, should only do so after medical consultation, though the enforcement of that would be just the kind of government interference that the right usually say they oppose. The government already wants to refuse children the right to be recognised as trans at school.
Finally, even a potentially sensible suggestion that those close to 18 should not have a sudden transfer to adult services but have a continuity of care after 18, has been met with suspicion from many trans people who fear it may be a means to restrict adult care, especially for under 25s. Such is the level of distrust.
Conclusions
It is crystal clear that in appointing Hilary Cass, the government would get the recommendations it wanted. She has done her job well. By dressing up the talking points of anti-trans campaigners in the language of academic neutrality and “care” she has given respectability to their prejudices. The mainstream media will now refer to the review as uncontested fact. Those questioning or opposing it will be further marginalised, especially trans people themselves. It has already been used to support calls for a similar review of adult gender services.
The Labour Shadow Health Secretary, Wes Streeting, who used to work for the main LGBT campaign group, Stonewall, has reneged on his support for trans people, as he has on just about everything else. He wasted no time at all in selling his soul by calling for the Cass recommendations to be implemented in full – in an interview with The Sun!!
The right are now baying for the recommendations to be enforced on private medical providers. They know that desperate trans kids and their parents will seek private treatment if they can afford it. But if that avenue is blocked then they will have no alternative but the black market, with all its obvious dangers.
Faced with such relentless negativity, many trans people are feeling despondent and powerless. These are dark times, and they will need to fight dogged trench warfare, case by case, issue by issue, to get the treatment they need. This needs to be part of a united campaign to secure decent funding for the NHS as a whole
At times like these, the labour and trade union movement needs to give its full support to its trans members and trans people in general – to stand up to the hate mob. The current right-wing campaign against the rights of trans people is part of a global phenomenon that is also aiming to roll back gay and lesbian rights and women’s rights across the board. The only weapon that working people possess is mutual support and solidarity, to overcome division and struggle for a better, fairer world, free of oppression.
[For more general articles on the trans issue see here and here]

